Dental Patient Reactivation Calls: A Script and Schedule
Dental patient reactivation calls that actually book appointments. The 90-second script, the 10-day call schedule, and exactly when to escalate or stop.
Share:
Table of contents
Dental patient reactivation calls work or fail based on two things, and the team almost never controls them: the script and the schedule. Get either wrong and reactivation rates collapse to single digits, the same range as text-only outreach.
According to the ADA, 20-30% of patients become inactive within 18 months without follow-up. Most of those patients can come back. They just need the right call at the right cadence, not a generic "we noticed it's been a while" voicemail that lands in the deleted folder.
This article gives you the 90-second script that converts, the 10-day call schedule that respects the patient and the contact list, the lapse-window math that tells you which patients to call first, and the operational rules for who should make these calls and when to stop.
What Should You Actually Say on a Dental Patient Reactivation Call?
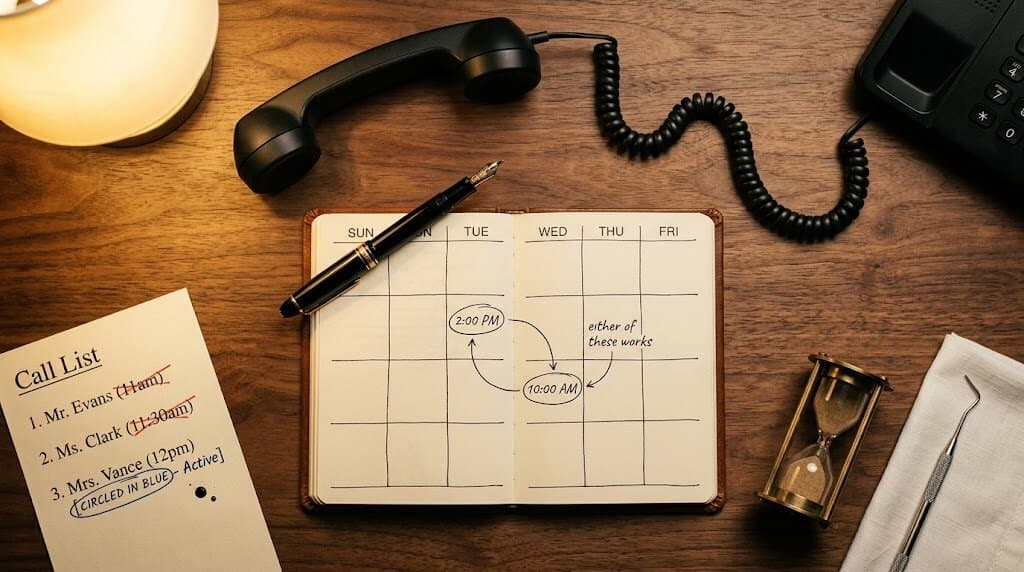
A working dental patient reactivation call closes in 90 seconds and follows four beats: open with the patient's name and last visit date, offer two specific time slots, handle one objection if it surfaces, then book or end. No filler, no apologies for calling, no reading "we noticed it's been a while" from a script.
The opening is the highest-leverage line. "Hi Sarah, this is Janet from Peterborough Family Dental. We had you in for a cleaning back in March 2025." That single sentence does three jobs: it confirms identity, anchors the relationship in real time, and removes the awkwardness of explaining why you're calling. Compare that to "Hi, we're calling because you're due for your appointment." The second version sounds like a reminder, not a relationship.
The 90-second script, beat by beat
- Open (10 seconds): "Hi [name], this is [your name] from [practice]. We had you in for [last visit type] back in [month, year]."
- Offer two slots (15 seconds): "We're booking up for [next month]. I have a Tuesday afternoon at 2pm or a Thursday morning at 10am — does either of those work?"
- Listen and handle (30-45 seconds): If the patient says yes, book. If they say "I've been busy" or "let me check," respond with one alternative or one reframe, not three.
- Close (15 seconds): Confirm the slot, tell them the SMS confirmation is coming, set the expectation for the visit length.
The single highest-leverage change in any reactivation script is asking for the booking before you hang up. Most callers don't. They give the patient information and tell them to "call back when ready," which adds a step the patient won't take. Dental Economics data on call-handling shows that booking-on-the-call practices reactivate at 2 to 3x the rate of practices that send patients to the website to schedule.

How Should You Schedule Reactivation Call Attempts?
Three call attempts over 10 days at different times of day, then one voicemail with an immediate SMS follow-up, then the patient cycles back into the queue 90 days later. That's the schedule. More attempts than three burns the contact list and produces complaint risk. Fewer than three caps your reactivation rate well below what the math allows.
The cadence works because patients don't pick up at random. They pick up based on patterns. A patient who didn't answer Monday morning may pick up Wednesday afternoon. A patient who didn't answer at noon may pick up at 5:30pm. Calling the same patient at the same time three days in a row is the worst possible pattern. It hits the same dead spot in their schedule three times.
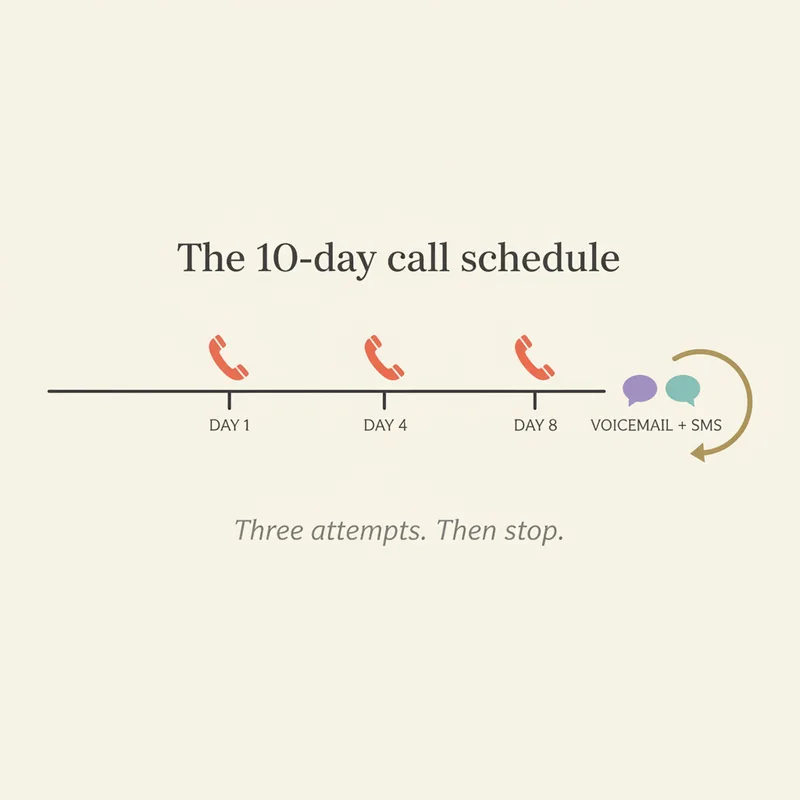
Why three attempts and not five?
Past three attempts, marginal pickup rate falls below 4% per call while complaint risk climbs sharply. According to BrightLocal data on consumer communication preferences, patients who feel "called too much" leave reviews that meaningfully damage local rank. The 90-day cycle exists to give the patient breathing room and keep your contact list clean.
Run the schedule consistently or skip it
Inconsistent reactivation cadence is worse than no cadence — it produces the worst of both: complaint risk and missed conversions. DentiVoice runs the cadence automatically so it never drifts.
See DentiVoice for reactivation →How Do Reactivation Rates Vary by Lapse Window?
Reactivation rates drop sharply with lapse length. Tier-one calls (6 to 12 month lapses, routine hygiene patients) book at 18 to 30%. The 12 to 18 month bucket drops to 10 to 18%. Past 18 months, reactivation falls to 5 to 10% and the call needs a different opening that acknowledges the larger gap.
That gradient matters operationally because it tells you which patients to call first. A 200-patient lapsed list isn't 200 equal opportunities. The 6 to 12 month bucket usually has the highest expected booked appointments per hour of calling time, even when the bucket has fewer total patients than the longer-lapse buckets. Sort the list by lapse window before you start dialing, not after.
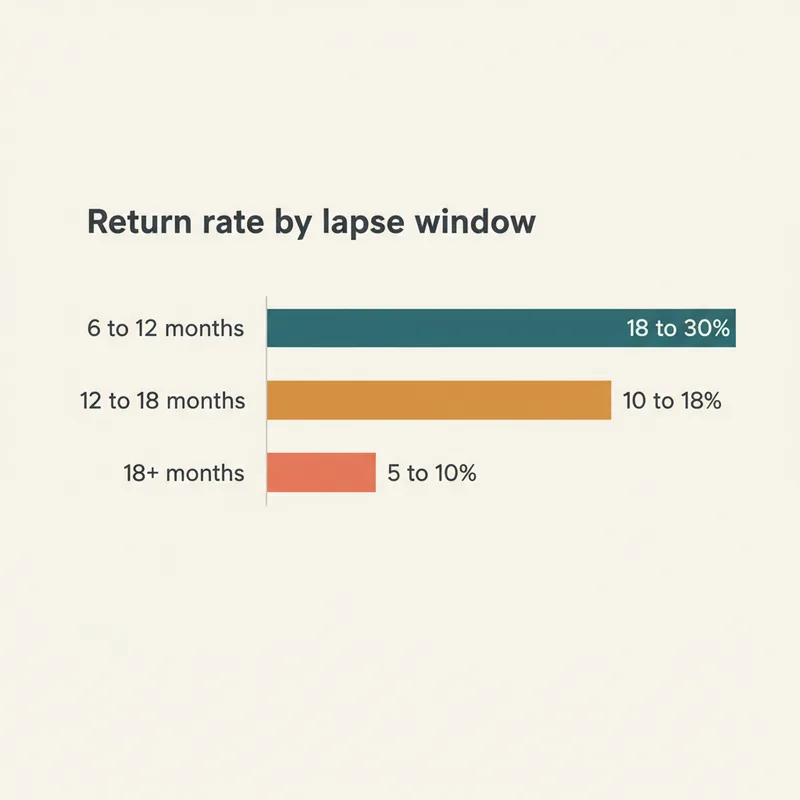
The pattern shows up clearly in Dental Economics data tracking reactivation outcomes across thousands of practices. The 6-12 month patients still remember you. The 12-18 month patients are evaluating whether to switch. The 18+ month patients have usually already switched, and the call is more about second-chance than reactivation.
How the script changes by lapse window
- 6 to 12 months: Standard opening with last visit date. The patient remembers; no need to over-explain.
- 12 to 18 months: Acknowledge the gap softly. "I see it's been a little over a year, just wanted to check in and offer you a spot if the timing works."
- 18+ months: Lead with relevance, not recall. "We're reaching out to patients who haven't been in for a while in case you've been thinking about coming back." This is no longer a recall call. It's a re-engagement call.
Who Should Make Dental Patient Reactivation Calls?
Reactivation calls should be made by a focused caller with no other duties during the calling block, ideally a senior front desk team member or a dedicated outbound caller. Front desk staff juggling check-ins, insurance verification, and inbound calls book reactivation at roughly one-third the rate of focused callers. The structure of the work, not the skill of the caller, is the variable.
According to Harvard Business Review, reactivating an existing patient costs 5 to 7x less than acquiring a new one through marketing, but only when the reactivation work actually happens. In most practices, it doesn't, because the people doing it are interrupted every 90 seconds.
Three operational models that work
- Dedicated outbound caller: Part-time hire whose only job is reactivation calls during a defined block. Highest reactivation rate per hour. Caps at roughly 100 calls per week.
- Batched calling blocks: Front desk team blocks two hours per day with no other duties (door locked, phones forwarded). Works for practices under 200 lapsed patients.
- AI voice for tier one: AI handles routine 6-12 month hygiene reactivation, human callers handle 12-18 month and high-value cases. Only model that scales past ~500 lapsed patients without adding staff.
Related: The decision between adding a human caller and adding AI usually comes down to lapsed-list volume and case mix. → AI Dental Recall Calls: When It Beats a Human Caller
When Should You Stop Reactivation Calls and Cycle the Patient Out?
Stop reactivation calls after three attempts and one SMS, then cycle the patient back into the queue 90 days later. Don't keep dialing. Patients past 24 months of lapse who haven't responded to two full cycles (six total call attempts plus two SMS waves) should drop off the active reactivation list and into a long-form re-engagement track instead.
The reason to stop matters as much as the reason to call. A clean contact list converts. A list patients have flagged as spam doesn't. BrightLocal data shows that perceived over-contact damages both reactivation outcomes and review reputation. The cost isn't just the unconverted patient; it's the next ten patients who see a one-star review about being called too much.
The cycle-out criteria
- Two complete cycles without contact (6 calls + 2 SMS over ~6 months).
- Patient explicitly opted out of phone outreach during any prior interaction.
- Patient lapsed 24+ months with no response to either cycle.
- Phone number returned as disconnected or flagged as a bad contact twice.
Move these patients to a quarterly email-only re-engagement track or remove them entirely. They're not coming back from outbound calls, and the calls are now hurting more than helping. According to the CDC, regular dental visit frequency among adults has stayed roughly flat for a decade, which means most lapsed patients went somewhere else, not nowhere.
Run reactivation calls without burning your front desk
DentiVoice runs the script and the schedule with no drift. Books directly into your scheduler, fires SMS fallback in 60 seconds, and stops calling exactly when the rules say to stop.
See how DentiVoice runs reactivation →What Does a Working Dental Patient Reactivation Calls Program Look Like Weekly?
A working program runs reactivation calls every week as a scheduled block, sorts the lapsed list by lapse window before each session, follows the 90-second script and 10-day schedule without exceptions, and reports outcomes by bucket so you can tune the script and the cadence based on real data. Not "we should do recall calls more." A standing operational system.
The weekly rhythm matters more than the volume. A practice that runs four hours of focused calling on the same two days every week reactivates more patients per quarter than a practice that runs ten hours one week and zero the next. Dental Economics reports that automated and well-run recall systems increase return rates by 25 to 40% over no-recall baselines, but the practices hitting those numbers all share the same structural feature: a fixed weekly block that doesn't get bumped for clinical work.
For a deeper look at where reactivation fits inside the broader recall system, the recall calls vs SMS analysis we published last week walks through the channel-mix decision in detail.
The Reactivation Decision That Actually Matters
The script and the schedule are the two levers. Most practices have a recall list. Most don't have a reactivation script that books on the call, and almost none have a 10-day schedule the team actually follows. Fix those two things, and reactivation rates move from single digits into the 18 to 30% range without any new technology, new staff, or new marketing.
If you only do one thing this month, write the 90-second script, print it, and ask every caller to follow it for two weeks. Measure the result. If reactivation rates jump and your team can sustain the calling volume, you have a working manual program. If volume is the constraint, that's when AI voice or a dedicated caller earns its place. Don't lead with the technology decision. Lead with the script.
See dental patient reactivation calls run end-to-end
Live demo using your script, your lapsed list, and your scheduler. 20 minutes, walks through the exact deployment. No commitment.
Book a Free Demo →Want more practical playbooks like this?
Browse Resources →Sources & References
- Patient Retention Statistics — ADA Health Policy Institute
- The True Cost of the Empty Chair — Dental Economics
- The Value of Customer Retention — Harvard Business Review
- Adult Oral Health and Dental Visits — CDC
- Local Consumer Communication Preferences — BrightLocal
- SMS Reminders and Healthcare Adherence — Journal of Dental Hygiene
Frequently Asked Questions
Open with the patient's name and last visit date, name two specific time slots ('Tuesday at 2 or Thursday at 10'), handle one objection if it surfaces, then book or end the call. Total target: under 90 seconds.
Three call attempts over 10 days, then one voicemail with an SMS follow-up. After that, cycle the patient back into the recall list for another attempt 90 days later. Don't burn the contact list with daily calls.
Tuesday through Thursday between 10am and noon, or 4pm to 6pm in the patient's local time zone. Avoid Mondays (full inboxes from the weekend) and Friday afternoons (people are mentally checked out).
Yes. Recall calls touch patients due for routine hygiene. Reactivation calls touch patients lapsed 12+ months who've drifted. Reactivation needs a softer opening, an acknowledgment of the gap, and a stronger value reason to come back.
Tier-one reactivation calls (6 to 12 month lapses, routine hygiene patients) book 18 to 30% on first contact. 12 to 18 month lapses drop to 10 to 18%. 18+ month lapses fall to 5 to 10% and require a different approach entirely.
Acknowledge it, don't argue with it. 'Totally understand. We've got Tuesday at 4pm or Thursday at 7am if either works around your schedule.' Most patients say 'busy' because they don't want to negotiate. Two specific slots remove the negotiation.
On the third attempt, leave one short voicemail (under 20 seconds) with your name, the practice name, and a callback number. Follow up immediately with an SMS offering the two time slots. Don't leave voicemails on attempts 1 and 2.
A focused caller with no other duties for the calling block, ideally a senior front desk team member or a dedicated outbound caller. Front desk staff juggling check-ins and inbound calls book reactivation at one-third the rate of focused callers.
Was this article helpful?
Written by
DentalBase Team
Expert dental industry content from the DentalBase team. We provide insights on practice management, marketing, compliance, and growth strategies for dental professionals.

